

Lymphatic Imaging (PDE Video Fluoroscopy)

What does a normal scan look like?
Normally, ICG is rapidly absorbed into the lymphatic system and transported up the lymphatic vessels to the lymph nodes in the armpit or groin. We can assess how quickly the ICG is absorbed and moved up the limb. As the PDE is real time imaging, we can observe the vessels contracting and pushing the dye towards the lymph nodes (peristalsis). A scan showing normal function shows the linear lymphatics with good progression of dye can be seen here.
There are 2 types of lymphoedema:
- Primary lymphoedema is a problem caused by failure of the lymphatics to develop. It can present at birth or in early or late adulthood.
- Secondary lymphoedema is more common and caused by damage to or removal of lymphatics as part of the treatment for cancer.
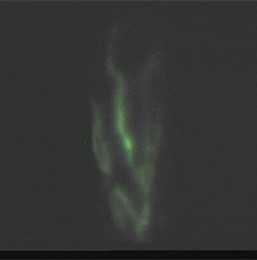
In secondary lymphoedema, there is a blockage to the normal flow of lymphatic fluid out of the limb. This leads to an increase in pressure within the lymphatic channels as they are unable to drain via the normal route. The increased pressure means that the fluid flows backwards into the microscopic lymphatic vessels that collect lymph fluid from the skin. The lymph fluid then leaks into the skin, which is called dermal backflow. This dermal backflow can be seen on the scan. As the lymphoedema worsens different characteristic patterns can be detected and recognised.
Early dermal re-routing is called ‘splash back’, but as the lymphoedema progresses it evolves into a more severe starburst pattern. In very severe lymphoedema, the dye collects throughout the skin and subcutaneous tissue, leading to a diffuse pattern.
In primary lymphoedema, the PDE picture varies depending on the type of primary lymphoedema. Some forms of primary lymphoedema are caused by absence of parts of the lymphatic system or lymph nodes, and therefore the ICG lymphography results are like secondary lymphoedema.
In other forms of primary lymphoedema there are abnormal or absent lymphatic channels. This is seen as severely delayed uptake and transport of the ICG or even totally absent uptake and transport.
How safe is ICG video fluoroscopy?
ICG has a robust safety profile as it is metabolised by the liver and does not rely on good kidney function to clear it. It can therefore be used in patients with renal impairment. Allergic reactions to ICG are very rare even with high doses and no episodes of allergic reactions have ever been reported following the low dose subcutaneous injections used for ICG lymphography.
There is a very small risk of introducing infection by giving injections into the arm or leg affected by lymphoedema, but this is unlikely as sterile needles and antiseptic skin preparation are used routinely. Antibiotics will be used in the unlikely event an infection occurs.
ICG lymphography does not involve exposure to radiation like lymphoscintigraphy. The dye has a green colour and may leave a small green patch of skin, like a bruise, for a few days following the test. After ICG lymphography, you can resume normal activities straight away, for example, it is fine for you to drive yourself home.

